COVID-19Test, trace & isolate.
|


|
The impact of an epidemic could be minimized by treatment of the disease or by avoiding spreading of the disease. In a virus epidemic, this means preventing contamination by infected people. In theory there are two ways to do this, first is to isolate everybody from everybody in a lockdown – i.e. extreme social distancing, second is to isolate all infected people. Isolating infected people requires testing in order to know who is infected with SARS-2. The most efficient testing strategy is to test diseased people or people at high risk and use confirmed cases to trace and test sources and contacts. All (putatively) infected persons must be isolated to prevent new contaminations. Test, trace & isolate (TTI) is the general strategy to fight virus epidemics. If the epidemic is under control by TTI, lockdown measures could be eased.
Infection without symptoms
Virologists know that not everybody will be diseased after an infection. An infection is defined as a contamination that yields virus production and could cause symptoms (WHO). Respiratory RNA viruses, like coronaviruses, are multiplied in the host (human) during the de presymptomatic phase – prior to onset of disease due to the immune reaction against the virus. Some people will never become ill, even though they’re infected, and remain asymptomatic. Asymptomatic and presymptomatic infection are documented in the medical scientific literature for most viruses, including SARS-2.
A systematic review estimated that 40% of SARS-2 infected adults remain asymptomatic, in spite of high virus titres (Gao). At a cruise ship 81% was asymptomatic (Ing), the difference may reside in monitoring general asymptomatic infection or asymptomatic infection with high virus titres. Almost 50% of the Dutch people does not notice their COVID-19 infection (Sanquin). In nursing homes, the care-givers oversee many people with high virus titres (AUMC). Also the care-givers have great difficulty to detect their own disease, not just of the elderly. Most likely, many adults could be infected with SARS-2 without clear symptoms. The head of the Dutch National Institute for Public Health and the Environment, Van Dissel, does not yet draw that conclusion. In children, virus emission could be measured for several weeks, without clear symptoms (Han, DeBiasi). Not everyone infected with SARS-2 will develop COVID-19, but most of those can contaminate others who could develop serious disease.
A systematic review estimated that 40% of SARS-2 infected adults remain asymptomatic, in spite of high virus titres (Gao). At a cruise ship 81% was asymptomatic (Ing), the difference may reside in monitoring general asymptomatic infection or asymptomatic infection with high virus titres. Almost 50% of the Dutch people does not notice their COVID-19 infection (Sanquin). In nursing homes, the care-givers oversee many people with high virus titres (AUMC). Also the care-givers have great difficulty to detect their own disease, not just of the elderly. Most likely, many adults could be infected with SARS-2 without clear symptoms. The head of the Dutch National Institute for Public Health and the Environment, Van Dissel, does not yet draw that conclusion. In children, virus emission could be measured for several weeks, without clear symptoms (Han, DeBiasi). Not everyone infected with SARS-2 will develop COVID-19, but most of those can contaminate others who could develop serious disease.
Test
Testing people without symptoms
Infected people without symptoms spread the epidemic. According to the Dutch governance, asymptomatic people have no reason to remain in quarantine. Virologists know that these people should be traced, tested, and if infected, should be quarantined. This is the default strategy for veterinary epidemics, and human viruses like HIV, SARS-1, MERS and Ebola. Rapid diagnostics, in the presymptomatic phase of infection, is crucial and the focus of governance.
Some countries only test people with symptoms, but others test everybody (Figure 1). Most European countries, the continent hit hard by the epidemic, test only people with symptoms. Germany and Greece, two countries with relative low levels of infection, test everybody. The Netherlands are inconsistent on testing without symptoms. It was advised against at August 26th, after being facilitated earlier (Figure 2). Just the day before, Sanquin concluded their paper: “This confirms the Healthcare service (GGD) advises: with health complaints everybody should be tested, and even without complaints everyone should cooperate with tracing contacts.
At September 5th, the GGD distances itself even more and says testing without symptoms could be harmful, since being tested may motivate reckless behaviour (Trouw). This kind of suggestion is not new, it was made before for HIV, but falsified by scientific papers (Aghaizu; George). Recently, this has been confirmed for COVID-19. Apparently, the new president of the GGD is unaware of this historical knowledge. The link to the Dutch soap-like discussion on mouth masks is obvious. In brief, the shortage of masks motivated the so-called scientific reasoning. Figure 3 shows that the interests of the OMT advisory board could overlap with their advices. Transparency of advises is crucial when conflicted interests are indicated.
Some countries only test people with symptoms, but others test everybody (Figure 1). Most European countries, the continent hit hard by the epidemic, test only people with symptoms. Germany and Greece, two countries with relative low levels of infection, test everybody. The Netherlands are inconsistent on testing without symptoms. It was advised against at August 26th, after being facilitated earlier (Figure 2). Just the day before, Sanquin concluded their paper: “This confirms the Healthcare service (GGD) advises: with health complaints everybody should be tested, and even without complaints everyone should cooperate with tracing contacts.
At September 5th, the GGD distances itself even more and says testing without symptoms could be harmful, since being tested may motivate reckless behaviour (Trouw). This kind of suggestion is not new, it was made before for HIV, but falsified by scientific papers (Aghaizu; George). Recently, this has been confirmed for COVID-19. Apparently, the new president of the GGD is unaware of this historical knowledge. The link to the Dutch soap-like discussion on mouth masks is obvious. In brief, the shortage of masks motivated the so-called scientific reasoning. Figure 3 shows that the interests of the OMT advisory board could overlap with their advices. Transparency of advises is crucial when conflicted interests are indicated.
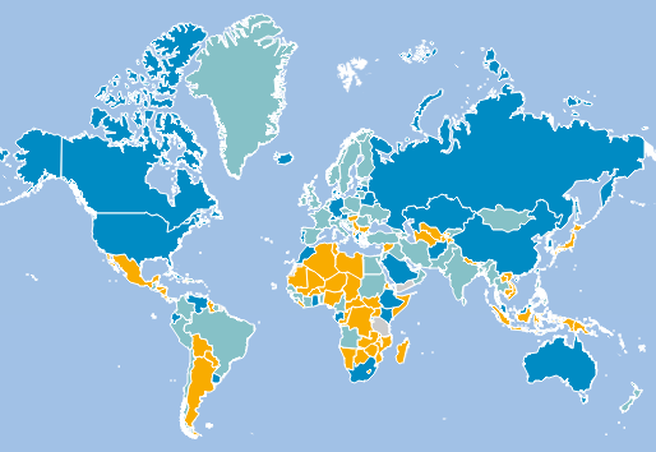
Figuur 1. International policy of testing. Grey no policy. Yellow only serious diseased people and target groups, turquoise everyone with symptoms, Blue everyone including persons without symptoms. (Volkskrant).

Figure 2. Official tweet of the Netherlands asking people not be tested without symptoms

Figure 3. Link at NVMM site to a paper in the Groene “Price fighting at the virus market.” The NVMM title "Commecial testing labs reduce the overview of physicians on virus epidemics. The NVMM experts are crucial in the OMT advice and have a conflict of interest in their medical microbiological labs.
Medical microbiology
The medical microbiology labs are not envied. They are essential in identifying new diseases with their added value in hospital diagnosis for therapy and treatment (Silven). Virologist, Bill Gates and this author warned for decades against putative new virus outbreaks. Against these warnings, the Dutch government has cut back on diagnostic labs for years, threatening the survival of the microbiological labs. Every year three new epidemics arise, and the majority is are caused by viruses. In this world with increasing (air) travel, more virus outbreaks can be anticipated. We must be prepared for that to limit the impact of a new epidemic.
Since early March, the medical microbiology labs are working overtime for SARS-2 diagnostics. This diagnostic capacity was insufficient in TTI context to prevent the epidemic from overflowing the intensive care (IC) units. Thus the Netherlands changed their triage from level 1 to 2, implying less elderly people at the IC, but fortunately could avoid level 3, in which patients with good recovery prediction would have to be denied access to the IC. Just like the TTI, the Dutch government forgets the diagnostic labour force that worked overtime not for three but six months to fight for the population health. So it is clear why the medical microbiologists are frustrated (NVMM).
However, the added value of medical microbiologists is limited for mass virus diagnostics in an epidemics. Other labs can do this more efficient. COVID-19 legitimizes the medical microbiologist, and the NVMM are tempted to confuse their own interests with national interests (Nieuwsuur). Because of many NVMM members in the Outbreak Management Team (OMT) a conflict of interest between their professional interests and the confidentially generated OMT advice arises (Ark). This can also be read in the NVMM correspondence with the ministry of Health. Obviously, transparancy is needed.
Since early March, the medical microbiology labs are working overtime for SARS-2 diagnostics. This diagnostic capacity was insufficient in TTI context to prevent the epidemic from overflowing the intensive care (IC) units. Thus the Netherlands changed their triage from level 1 to 2, implying less elderly people at the IC, but fortunately could avoid level 3, in which patients with good recovery prediction would have to be denied access to the IC. Just like the TTI, the Dutch government forgets the diagnostic labour force that worked overtime not for three but six months to fight for the population health. So it is clear why the medical microbiologists are frustrated (NVMM).
However, the added value of medical microbiologists is limited for mass virus diagnostics in an epidemics. Other labs can do this more efficient. COVID-19 legitimizes the medical microbiologist, and the NVMM are tempted to confuse their own interests with national interests (Nieuwsuur). Because of many NVMM members in the Outbreak Management Team (OMT) a conflict of interest between their professional interests and the confidentially generated OMT advice arises (Ark). This can also be read in the NVMM correspondence with the ministry of Health. Obviously, transparancy is needed.
Test to fight the epidemic
Early on, I made a simplified model for COVID-19 based on my estimation for R0, basic reproduction number of the virus epidemic. Using international studies, I estimated R0 = 3.6, which explains the rapid growth in the number of Dutch cases better than the official estimate of R0 = 2.2. The Netherlands had to tighten lockdown measures repeatedly, since the virus spread more rapidly than officially predicted.
Figure 4 shown how theoretical epidemic growth without measures, when only diseased people are isolated, and when all infected people are isolated. Only isolating all infected people could stop an epidemic. Figure 5 illustrates the same method in a graph.
Figure 4 shown how theoretical epidemic growth without measures, when only diseased people are isolated, and when all infected people are isolated. Only isolating all infected people could stop an epidemic. Figure 5 illustrates the same method in a graph.
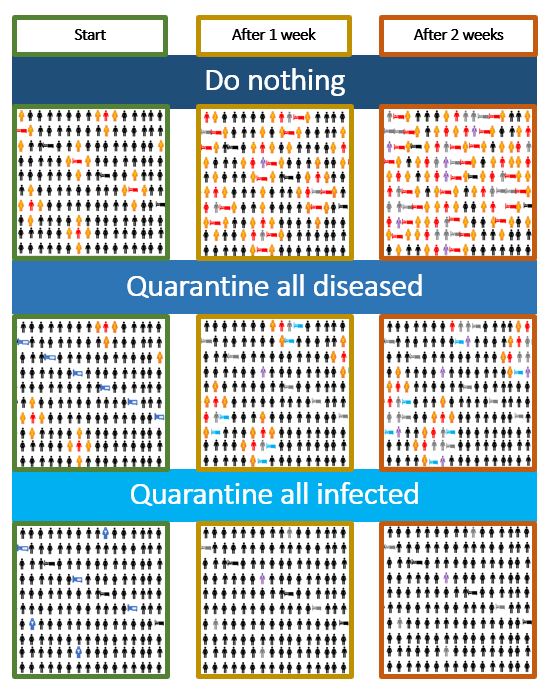
Figure 4. Efficiency of different strategies on the development of the epidemic. Up to down are three different strategies depicted with theoretical 100% efficacy: (i) do nothing against the epidemic, (ii) isolate all diseased people and (iii) isolate all infected people, with or without disease. Red indicates infected people, yellow new contamination, blue isolated infections, purple deceased persons. grey recovered persons. Beds indicate diseased persons.
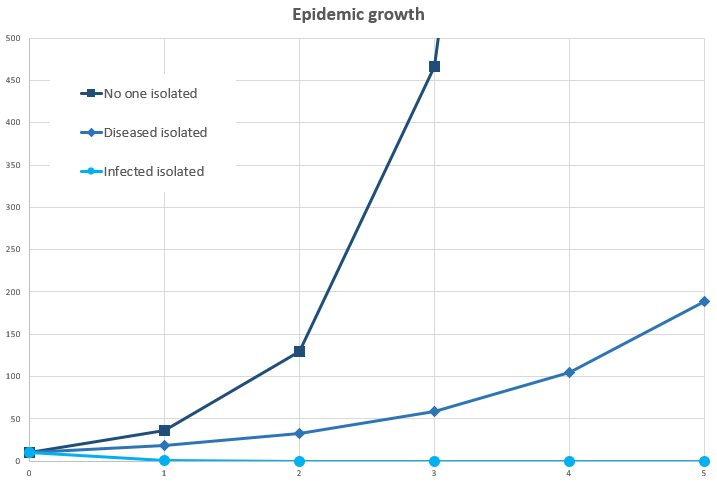
Figuur 5. Graph with epidemic development in three different strategies
Is testing efficient?
Physician-microbiologist Alex Friedrich (UMC Groningen) criticizes the Dutch policy: “We did not adhere to our national policy and test all the care-givers.” We know that an infected care-giver could contaminate 20 to 30 patients and co-workers. He aims to stop the epidemic early on by testing frequently (Groene). An evaluation showed that this different policy correlates with less infected people, less hospitalizations and lower death rates in the population of Groningen (Hoekman).
Also the independent experts in Lessons learned advise to implement test, trace and isolate completely. To avoid misunderstanding, it is not urged to do a full population screening, like Luxemburg does. The Netherlands are clearly not prepared fort hat, and populations with a very low risk have a relative large risk for false positive results. Population screening would require rapid tests. Their advice is to trace the source and all contacts of each infection. Furthermore, people in contact with other people, like care-givers, working in regions with a relevant incidence of infections, should be tested for COVID-19. The threshold of the incidence would depend on the intensiveness and frequency of the number of contacts. Controlling a virus epidemic is harder when the infection rates are high than when a population is almost devoid of infections. Virus epidemiologist always recommend to aims for zero infections. One should never aim at herd immunity against a virulent virus.
Also the independent experts in Lessons learned advise to implement test, trace and isolate completely. To avoid misunderstanding, it is not urged to do a full population screening, like Luxemburg does. The Netherlands are clearly not prepared fort hat, and populations with a very low risk have a relative large risk for false positive results. Population screening would require rapid tests. Their advice is to trace the source and all contacts of each infection. Furthermore, people in contact with other people, like care-givers, working in regions with a relevant incidence of infections, should be tested for COVID-19. The threshold of the incidence would depend on the intensiveness and frequency of the number of contacts. Controlling a virus epidemic is harder when the infection rates are high than when a population is almost devoid of infections. Virus epidemiologist always recommend to aims for zero infections. One should never aim at herd immunity against a virulent virus.
Can the Netherlands test sufficiently?
The Dutch news repeats the question of some that we cannot test enough because of lack of reagents. Friedrich says: “We do not have a capacity problem. A certain lab could lack some materials, but that is business as usual, is should be solved. One should never depend on a commercial partner. We do not need a commercial partner, since any lab could do these tests.” Also my own experience clarifies, “Yes, we can test! This is confirmed by the larger test labs in the Netherlands, like Sanquin and Eurofins, and those in Germany – which will be hired for Dutch testing. The real problem is not lack of reagents, but of validated reagents. This might imply some additional lab work to make solutions and validate reagents and consumables for the lab. Labs with limited employers could have a challenge there. But the difference between extra work and impossible to do should be solvable to halt an epidemic that costs billions of euros.
Test early
TTI requires rapid and efficient testing. RT-PCR diagnostics takes about 2 to 3 hours in a laboratory – excluding transportation of the ample to the lab. IT-technology, like LogiqCare, allows instant automated communication of lab results to tested persons.. So there seems to be no reasons that people should wait for more than 24 hours on their test results. Tiered test approaches using pre-screening are even more efficient, allowing over 90% of the diagnostics to be performed within minutes.
Trace
Trace to avoid inefficient testing of everyone *
Superspreading is often caused by persons unaware of their infections – often without symptoms. Testing the whole population will not work. The incidence of infections is probably lower (<0.1%) than the incidence of true positive (<1%), resulting in a high percentage of false positive results (zie tests). Infected persons could be traced though their contact with other infected cases. Source and contact tracing are two related but different strategies with different aims, which are most often combined in practice.
Trace the source
Source- and contact tracing are two related but different strategies with divergent aims. Source tracing starts at the tested person and aims to find the source of infection to provide insight in how much we know of the epidemic. Because of a fairly rapid mutating SARS-2 RNA, approx. 1 nucleotide per 10 days (WHO), the contaminating source can be identified and confirmed. Without continuous full population never a complete picture of the epidemic arises, and so some contamination might not be traceable to a (known)source. This will allow us to find new contamination sources, including putative superspreaders – and quarantine these.
Newly identified sources are a valuable insight of the epidemic below the surface. When 50% of all new infections reside from a (previously) unknown source, than over 50% of the epidemic is under the surface. The actual fraction will be higher, since unknown infections might also cause unknown contamination. As is said: “You don’t know what you do not know” (Figure 6). Estimating how much we do not know is crucial to estimate the risks of the epidemic, since it is very difficult to check unknown risks.
Newly identified sources are a valuable insight of the epidemic below the surface. When 50% of all new infections reside from a (previously) unknown source, than over 50% of the epidemic is under the surface. The actual fraction will be higher, since unknown infections might also cause unknown contamination. As is said: “You don’t know what you do not know” (Figure 6). Estimating how much we do not know is crucial to estimate the risks of the epidemic, since it is very difficult to check unknown risks.
Trace contacts
The second line of source and contact tracing is tracing the contacts. Contacts are persons with a high likelihood to be contaminated and infected. The speed of tracing contacts determines the efficiency of the TTI strategy (Kretzschmar). Every day delay reduces the efficiency considerably. This also includes testing presymptomatic contaminated persons later. Researcher Numan uses data from Covid Radar. He indicates hat it is difficult to motivate people to be tested quickly. (AD).
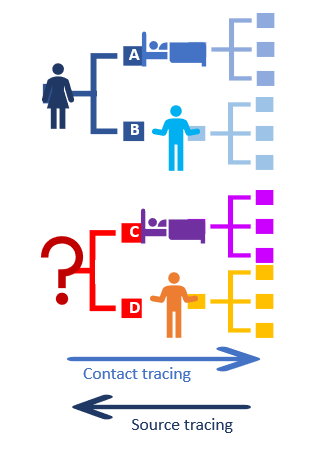
Figuur 6. Source- en contact tracing. A is known case with known source, B new infection detected with contacts. C. new case with unknown source. D unknown case with unknown source
How does it work? *
Virus infection spread from person to person. Tracing will look at contacts of persons around the infection. Source research traces the contacts prior to contamination (Figure 7). If the infected person now is virus-free, an antibody ELISA test could be helpful to show recent infection.
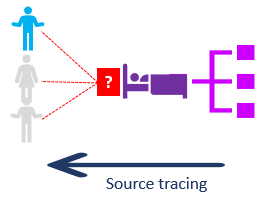
Figure 7. Tracing the source
New infections from the source *
Virus epidemics are difficult to control due to unnoticed asymptomatic infections. Whole population testing often results in many False-positive test results. The tracing methodology aims to find the infected persons. Starting with an infected case allows tracing the source (see previous), even if this one is asymptomatic. Newly detected sources would allow to uncover new contacts of these (Figure 8)
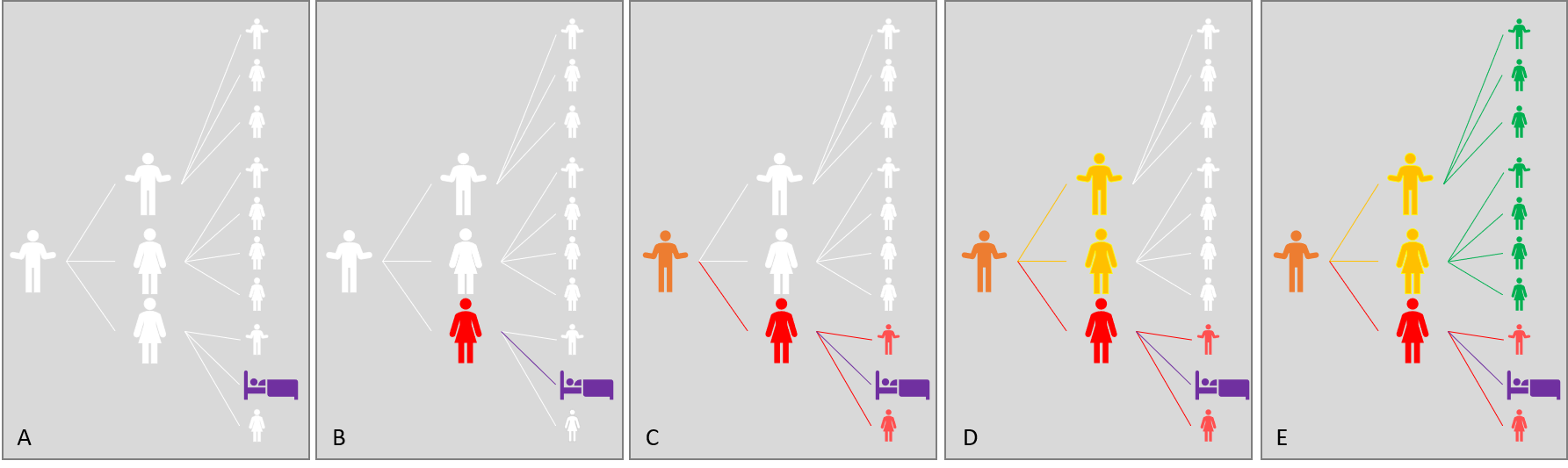
Figure 8. Tracing procedure. A. Infected case without source. B. Detection of source C. Finding source of source and new contacts of source. D. Finding contacts of deeper source. E. Finding contacts of contacts .
Isolate
Quarantine infected people
People who are ill will self-initiate to remain in quarantine. Having (serious) fever, (serious) breathing problems and/or a lot of coughing will motivate strongly not to go outside. Diseased people rely on their environment for care. Some people are not ill, but (possibly) infected. This could be by contact with infected people, e.g. at work, study and/or visiting a high-risk area. People with increased risk should be obliged to be tested. The current Dutch regulations are complex and based on risk estimation, not on infection. More testing is needed to motivate people to remain in quarantine.
Quarantine is less appealing for people without COVID-19, because it affects work, study and recreation. Unnecessary quarantine causes much discomfort, including for the 1 million people in the Netherlands with a lung disease.. How could this be prevented?. Testing is crucial, the more specific a test is, the less the risk of unjustified isolation.
The Netherlands have not obliged quarantine because the Chamber majority considers this a too strict an approach for uncertain infections. Within the context of obligated source and contact tracing, testing for being virus free would regain freedom. A precondition for such a legislation is that everyone could be tested and have their results within 24 hours.
Quarantine is less appealing for people without COVID-19, because it affects work, study and recreation. Unnecessary quarantine causes much discomfort, including for the 1 million people in the Netherlands with a lung disease.. How could this be prevented?. Testing is crucial, the more specific a test is, the less the risk of unjustified isolation.
The Netherlands have not obliged quarantine because the Chamber majority considers this a too strict an approach for uncertain infections. Within the context of obligated source and contact tracing, testing for being virus free would regain freedom. A precondition for such a legislation is that everyone could be tested and have their results within 24 hours.
Good TTI provides freedom
Test, trace and isolate is the only way to minimize COVID-19 and all other epidemics. Testing should be fast and complete for presymptomatic and asymptomatic infections (Figure 9). Likewise for tracing. A good TTI strategy could fight the epidemic without requiring a lockdown.
Virologists only require infected people to be isolated, not the whole population. Most people are infected for two weeks or less, only who is diseased for a prolonged time should remain longer in quarantine. This could be a sustainable strategy against COVID-19, even if no safe vaccine is developed, and everyone, just as with the corona common cold viruses, is at a renewed risk, never allowing herd immunity to arise.
Virologists only require infected people to be isolated, not the whole population. Most people are infected for two weeks or less, only who is diseased for a prolonged time should remain longer in quarantine. This could be a sustainable strategy against COVID-19, even if no safe vaccine is developed, and everyone, just as with the corona common cold viruses, is at a renewed risk, never allowing herd immunity to arise.
Figure 9. "Tested this afternoon and received the result this evening!" (Twitter)
John Jacobs
12 - 09 -2020
* 26-09 -2020
12 - 09 -2020
* 26-09 -2020
